Recent Posts
Search the DAFNE Online Forums
15,751 posts found
|
Apr 18, 2013
mum2westiesGill
502 posts
|
Topic: General Discussion / 7-day waking average 6.3 - bedtime10.5 - this morning - 19.22pm - tea & QA - BG was 6.3 - 22.23pm - bedtime test was done |
|
Apr 17, 2013
youone
102 posts
|
Topic: General Discussion / Dealing with large carb meals
QA: Humalog BI: Lantus |
|
Apr 17, 2013
youone
102 posts
|
Topic: Carbohydrate Counting / Carbohydrates help needed - ASDA Ready Sliced Tiger Chest
When your at home weighting is the easy option if you know the gram value The method I used before the smart phone apps appeared is this ,it might be of use to you If your BI is set right and your used to carb free meals try this Cut a slice of the tiger bread which you would normally eat Take BG retain the reading done't take any QA re test 2 hours later that should be the highest reading and cross check after 4 hours if its constant compare the two readings what ever the correction is to bring it back to the reading 4 hours previous is the amount of CP the tiger bread was If you weighted the bread you now have a value you can use. Seems along about way of doing it but it worked for be.I still do this if I come across a food which isn't listed anywhere Especially my mothers baking |
|
Apr 17, 2013
paulj
36 posts
|
Topic: General Discussion / Dealing with large carb meals be careful to bear in mind that some q/a insulin you take i.e. novo-rapid can have a effect on your bg levels for up to 5 hours after intially taken. i think! so therfore if you take a reading after say 2 hours this may be giving you a false picture.but everyone is different i guesscheers |
|
Apr 17, 2013
youone
102 posts
|
That's great news Gari, just test every 2 hours until after a 8 hour period has passed, since this is a new method for you, where all different keep passing the info on |
|
Apr 17, 2013
Gari
17 posts
|
Youone thankyou thankyou thankyou. Thanks so much for your advice. I tried today. Had 23cps worth gave 8iu and then 7iu 2 hours after and now 7pm and my levels have been stable around 5mmols for the last hour. Once again thankyou so much. |
|
Apr 17, 2013
Apollo
45 posts
|
Topic: Questions ? / novo-rapid insulin duration Hmm sounds impressive.I'll pass on trying it out myself as I've got meters coming out of my ears. Last time I asked Bayer for a contour USB they sent me two of them plus a non USB model so I could almost have a different meter for every room in the house & they are asking me if I want the new latest model now. But it sounds like it has had a lot more thought put into it than I initially gave it credit for. I'll add it to my reading to do list |
|
Apr 17, 2013
novorapidboi26
1,818 posts
|
Topic: Questions ? / novo-rapid insulin duration Obviously these meters, and all the insulin pumps that provide on board insulin calculations, require an initial set up where you input the duration of your bolus/QA insulin......so they are real world tools in that sense, they are used and with a high reliability......have a look online at these meters.....you could probably get one free to try out......You would need to work out the insulin duration for each individual by testing, but I personally was put on a 4 hour duration when beginning with the pump, I have now increased that to 4:30 hours..... its pretty reliable, but as I mentioned before, if the carb count is correct and the duration has been fine tuned, you shouldn't ever need to give additional correction when eating in between the usual meal times.... |
|
Apr 17, 2013
Apollo
45 posts
|
Topic: Site Development / Figure 17 Sorry Marke,No offense meant, a really good friend of mine is an Aussie and we often make light hearted digs at eachothers expense so it was intended as friendly banter rather than an offensive remark. I take the point that its not always easy to tell the difference between sarcastic humour and abuse with a text based forum though so I'll be sure to be more mindful of it in the future. If it's any consolation I have been beaten into accepting that the fruit from a pepper plant is called a capsicum rather than a pepper ;) |
|
Apr 17, 2013
marke
655 posts
|
Topic: Site Development / Figure 17 Hi, can we avoid stuff like the last post please or I will just delete offending posts. This is a diabetes website not a bash other users website. Last time I walked down an english high street at night, there were plenty of people with a strange approach to class and sophistication |
|
Apr 17, 2013
Apollo
45 posts
|
Topic: Questions ? / novo-rapid insulin duration Interesting, I didn't know that there were meters that did that, I'd personally take what they say with a little suspicion though as the real world data compared to the graph I posted is roughly similar but no where near as smooth and perfectly predictable. It's the kind of feature I'd expect to come with a massive disclaimer and be more intended as a gimmicky little feature than real world tool.If in doubt (especially when operating a car, bike or bus) always safer to run high. I imaginr it was hard getting the ok to drive a bus as it is so you don't want to be giving anyone any reason to want to revoke your license by start hypoing |
|
Apr 17, 2013
Apollo
45 posts
|
Topic: Site Development / Figure 17 Aussies think a lot of odd things, for example drinking Stella is considered a sign of class and sophistication rather than domestic violance. |
|
Apr 17, 2013
novorapidboi26
1,818 posts
|
Topic: Site Development / Insulins great idea....... |
|
Apr 17, 2013
novorapidboi26
1,818 posts
|
Topic: Questions ? / novo-rapid insulin duration Great explanation by travler there.......If you do have to eat within the 4 - 5 hours you would simply take insulin for the meal without considering a correction, so you don't really need to test your blood sugar at this intermediate meal/snack.... however, there are now several meters on the market: Accu Check combo, InsulinX, which have a bolus wizard and on board insulin calculator on them.......these can tell you how much insulin is actually left in your system and whether or not you need some correction or not...... provided your carb count is correct and the insulin action is behaving as you would expect, there will never be a need to correct mid meal, as the wizard should work out that the correction you need for the 'mid meal' snack is in fact what is left in your system at that time...... |
|
Apr 17, 2013
mum2westiesGill
502 posts
|
Topic: General Discussion / 7-day waking average Tue 16/048.9 - bedtime 3.6 - this morning - 18.11pm - tea & QA - 22.41pm - bedtime test was done - treated this mornings hypo with 4 jelly babies then 15 mins later BS was 5.0 Wed 17/04 14.5 - bedtime 10.2 - this morning - 18.58pm - tea & QA - 22.42pm - bedtime test was done |
|
Apr 17, 2013
Gari
17 posts
|
Thanks you one I like your way of thinking. I think I will try this today at lunch I will report back and let you know how it goes. Fingers crossed for me. |
|
Apr 17, 2013
Gari
17 posts
|
Topic: General Discussion / Dealing with large carb meals Hi travlerMy normal time is just before I start eating my meal. The kind of meals include all takeaways and any meal with some carbs e.g bout 8 to 10 cp's plus dessert of maybe 5 to 7 cp's. I take novo rapid and a single dose of lantus. |
|
Apr 17, 2013
Warwick
434 posts
|
Topic: General Discussion / Dealing with large carb meals I can't take more than 8 units of QA at a time without hypoing, so I also split my doses for very high carb meals. I usually test 2 hours after the first injection and correct any high value at that time to take my BGLs down to 8.0. That gives me a bit of leeway with the QA already on board.I find I also need to do this with slow-release foods like beans, chick peas and lentils. It feels a bit odd injecting QA when my BGLS are in the 5s before bed after a Nachos dinner, but I forgot to do this correction a couple of nights ago and had BGLs of 12.5 before breakfast after going to bed with BGLs of 5.8. The times that I have remembered, I've been fine overnight and woken with normal range BGLs. |
|
Apr 17, 2013
Warwick
434 posts
|
Topic: General Discussion / Increased blood glucose after exercise Anaerobic exercise happens at high intensity, so if your cycling was at high intensity both ways, then that would be anaerobic, but if it is the sort of cycling that you could whistle a tune while riding, then it will be very aerobic instead.I cycle to and from work each week day, (an hour each way, gradual uphill on the way to work, nice and downhill on the way home) and my BGLs follow the pattern of aerobic activity. It is fairly rare that I cycle with intensity - having a newborn in the house means I am too sleep-deprived to feel energetic enough :-) I never hypo on the way to work because it is within a couple of hours after breakfast and I have both carbs and QA on board, but I do have to be careful in the hours afterwards until lunchtime. Going home, I have to eat before cycling or I will with 100% certainty hypo. I could lower BI, but it tends to lead to highs at other times, so I don't. I'd suggest that you don't take additional QA unless you see a definite pattern of highs after cycling. If you do, then you can cautiously increase your QA before cycling, but one-off rises in BGLs do happen, especially with new activities so you may not see that again. Take care, Warwick. |
|
Apr 16, 2013
Apollo
45 posts
|
Topic: Questions ? / novo-rapid insulin duration Hi Paul,just another bumbling graduate rather than a HCP here but I think it's pretty hard to give set guidelines on how much of your insulin is spent and how much is still working. as a VERY rough guide there is the graph in the DAFNE handbook which I suspect you have seen already as some of what you said is almost a direct quote from it. 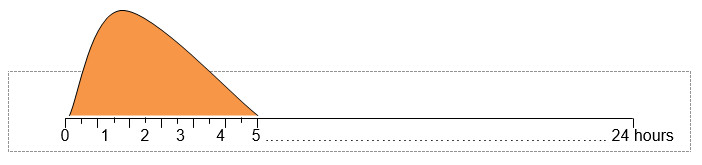 As a rough guide though you can see by hour 3 there is very little life left in it and by hour 4 you can almost assume it's all gone as a general rule. There are however a number of factors that can change how quickly the insulin will work, some are down to your physiology, some are environmental so that can only ever be taken as a rough guide and certain not something to do precision maths with to keep you just above 4mmols Personally I try to keep 4 hours between meals but if I had a late breakfast and can't push back lunch so there has only been 2 hours between the meals and I test and find I'm high, I choose to trust that I gave enough insulin earlier and it will bring me back down given time to finish working and take only the insulin that my lunch dictates (i.e. no correction) If I were you then should I find myself eating again less than 4 hours after my last shot I'd test, eat & inject without correction for any highs (obviously correct if there is a low) and then test again in 4-5 hours time and correct if required then. Also should you find yourself a bit close to the 4 mark the quickest way to get your levels up is with a sugary liquid, personally I go with a can of coke which I find hits the blood in under 5 mins. Not sure that's quite the advice you were looking for but I think there are probably a few to many unknowns to do exactly what you hoped to do, that said after a few months you may find you get a better understanding of how you personally react to the insulins you use and you may be able to refine things slightly better. Another thing that may be worth while to you is a continuous glucose monitor, which is a test meter you leave attached to you and tests every few minutes. Most have the option to then alert you if you're going low so you can prevent yourself going under 4mmols. I'm not sure if these are available on the NHS or not though so there may need to be an element of self funding on your part if this was something you wanted to look into. certainly asking you diabetic healthcare team what your options are with it though, they do tend to be expensive though. |
|
Apr 16, 2013
Apollo
45 posts
|
Topic: Site Development / Insulins I'm on a motorbike forum and we have it set up so that we can put what bikes we have under our user name in forum posts. This is useful as if someone starts saying "on my bike I..." you know without them needing to point it out what kind of bike out is and how better to advise them or how their experience relates to what you were asking about.As such I wondered if we could set it up so that we could list what insulins we are on in the same way? Or as a signature file. In fact a signature file would be brilliant to as every time I give someone an opinion I find myself wishing I could turn on a signature that said something like "I'm guessing here as much as you are if it makes sense then take the advice at your own risk, if it doesn't then talk to a medical professional" |
|
Apr 16, 2013
Apollo
45 posts
|
Topic: General Discussion / Dealing with large carb meals When is your normal time?I know some take it before the meal, while others like myself prefer after so they have a better idea of how much carbs they have consumed. If your in the former group then taking the shot after would mean that your BG levels would already be slightly elevated which may help counter the fact that the sugars are being released more slowly. Can you give some examples of the kinds of meals you experience this with? Also what insulins are you on? If your BI is levemir is it split? As the release of sugars 4 hours after meal sounds to be very slow and this most often occurs with your evening meal have you considered putting one or two extra units of your BI in to deal with it as the slow release pattern seems to better match the sugar release profile you mention and I'm wondering if the large meal is actually having an impact on your metabolism and what your experiencing is actually fat being burned to BG rather than carbs. Ì know when I have a hot curry that I have to put in a few extra units than the carbs there would typically suggest. If it is metabolism in your case then a great way to slow it down is alcohol... |
|
Apr 16, 2013
youone
102 posts
|
Topic: General Discussion / Dealing with large carb meals HiThis is the issue I've tried to understand and control like yourself over the years I've tackled it in different ways until I settled on an option similar to what Dafne teaches us. The method which I use is based on my experience over the 40 years i,'be been type 1, I guessed that it wasn't the amount of CP's I was taking it was the amount of insulin QA, I had no knowledge of Dafne or their principal's, but I took an educated guess that my body couldn't use the amounts of insulin I was taking in response to large meals of CP's. In response to this I set a limit of 10 units of QA maximum I would inject at a time. Hence a very large meal of 240 carbohydrates this was the way I controlled by condition before Dafne. My QA would be split into 3, 10 before meal 10 after the meal usually 2 hours then after 4 hours I would do a BG and do a correction, I use the word correction because of Dafne, I responded to the BG test, if it was OK I didn't inject if it was high I did. I found this method of drip feeding small amounts of QA worked or in other words my body could cope with the amounts of QA and was able to use it, I may have been just lucky that the amount I settled on 10 was right for me, where all different, Now with Dafne I use a lower number since I know now that 1 unit of QA will bring down my BG by 2 to 3 So for example if I had 18 CP's Soon as I have ordered I would take 6 QA if my ratio was 1:1 Two hours later I would take or when the meal had finished after a test 6 more QA Finally 4 hours after again re a BG reading I would correct Most occursions I would have to take the full 6, but I find the drip method gives me least chance of overkill and going into a hypo spiral. This method only differs from ture Dafne to the point where you inject before you eat but we all carry something for low BG and if the group or party your with know your a type1 it shouldn't be an issue,since I've sometimes taken a CP while waiting for the meal to come. I don't think there's an ideal way in tackling really high CP meals since I believe your body can only use so much QA at a time. Saturation occurs and like a flood you may experience a hypo later on. I'm not an expert and may be totally incorrect, but it worked for me Like you I'm very interested in other members views and methods to control large CP meals I look at it like this, we all eat about 20+ CP's a day you control this by taking your QA to match your CP intake at a meal usually 3 meals By doing this when taking similar amounts of CP's at once, by splitting your QA by 3 over a period you give your body a chance to use it correctly. |